
We Have a Duty to Find, Assess, and Support Twice-Exceptional Students
Summary of Significant Studies on High Suicide Risk for those with Autism/ADHD and the Heightened Risk for Those With Higher Cognitive Abilities


Research has established that there is a heightened risk of suicide in the neurodivergent population. Neurodivergent is an umbrella term that describes people with variation in their brain functioning, and can include conditions such as autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder (ADHD), dyslexia, dyscalculia, dyspraxia and tourette’s syndrome. The neurodivergent population is often at risk for a wide range of additional health risks leading to a lower life expectancy, health and mental health issues and overall lower quality of life. These health concerns are often exacerbated by 1) being misunderstood and unaccommodated by our neurotypical society institutions and systems and 2) sensory overwhelm. It is therefore not surprising that recent research has shown that the risk of suicide is significantly higher for autistics and ADHDers overall.
Many autistics often have additional conditions under the neurodivergence umbrella. In medical terms, their autism is comorbid with additional diagnoses[1]. Often the comorbid condition, ADHD, OCD, major depression,dyslexia, etc, is first diagnosed, and the formal ASD diagnosis arrives much later (or not at all) as it requires special clinical screening that is expensive and often comes with long-wait times of six months to over a year in some cases. Research studies consistently find heightened risk of suicidal behaviours, ideation, attempts and deaths in those with ASD and ADHD, especially if they are un or misdiagnosed. From the research, the risk of suicidality is higher for those with ASD and higher cognitive abilities, and even higher for those with ASD and other comorbid conditions. The risk of suicidality is higher yet again for those that are twice exceptional, defined as high IQ (>120) combined with another disability, such as ASD[2],[3].
To Support, We must Identify
Those with ADHD and ASD that are at the highest risk of failure to identify are those with higher cognitive functioning and compensation skills. It is obviously much easier to identify a non-verbal child. Being autistic comes within a wide spectrum of differing ways of being and often different subsets of mortality risks depending on their way of being. For example, the mortality risk for suicide is even higher for neurodivergents that are LGBTQ+ and/or for those with autism and/or ADHD and higher cognitive abilities. While it was previously thought that higher cognitive ability was protective, research has shown that with autism exactly the opposite is true - higher cognitive ability is significantly related to more suicidal thoughts and deaths in autistics. Higher cognitive functioning in ASD is often defined as greater than 70 IQ. The subset of population of “twice exceptional” children, or children who are “gifted” (higher than 120 IQ) with a “learning disability” (neurodivergent) are at much heightened risk of suicide or significant mental health issues when they are not assessed, identified and supported adequately. It is precisely these neurodivergent boys and especially girls, that are failing to be identified. They are often identified late in life, maybe after their unaccomodated disability spurns a suicidal mental health crises, or tragically not at all. They form a “Lost Generation”.
Suicidality Starts Earlier in Autistics - Schindel Letter
Suicidal, thoughts, & behaviors (“STB”) seem to arrive shockingly earlier in those with ASD (as young as 8)[4]. Reported lifetime STB incidence was as follows: 392 (40.5%) reported wanting to die, 187 (19.3%) reported wanting to end their own life, and 72 (7.4%) reported having a suicide plan. Among those answering affirmatively to each of these questions regarding STBs, onset at 8 years or younger was reported in 142 (36.2%- wanting to die), 66 (35.3%- wanting to end their own life), and 13 (18.1%- a suicidal plan) children, respectively[5].
This study was conducted in those that were clinically diagnosed with ASD and not those who are undiagnosed and/or misdiagnosed[6]. This study is also based on their caregivers’ report, which may understate suicidality, as it requires the caregivers to know what is internalized to the child despite autistics’ known difficulties with communication and (heightened or lessened) sensory perceptions, interoception and alexithymia[7].
The Swedish Study.
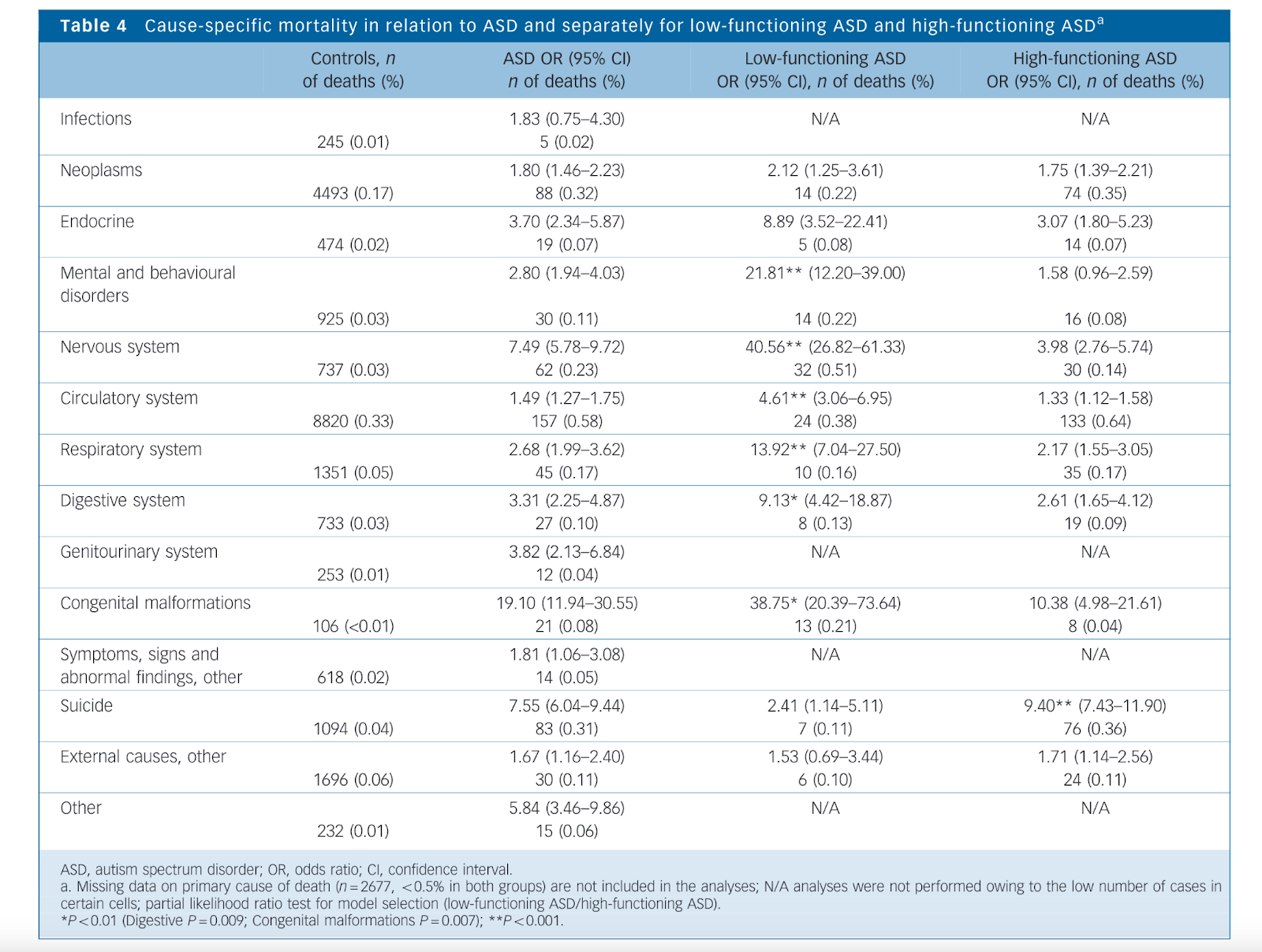
This research indicates a higher overall mortality rate in individuals with autism, including from cardiovascular, epilepsy and respiratory illnesses[8]. The overall mortality risks from this study were especially pronounced in those with low-functioning ASD (lower cognitive abilities) and females[9]. Additionally, ASD overall comes with increased risks of death from suicide[10]. The Swedish Study, covered diagnoses from 1987-2009, and shows mortality rates in the ASD population are significantly higher (2-3x) than the general population[11]. The study also found a much heightened risk of suicide in high-functioning ASD at 9.4x the general population[12]. For the unaware, high-functioning ASD more or less encompasses what was previously diagnosed as Aspergers with autism with higher cognitive abilities often measured as >70 IQ. It should be noted that when one hears the word “high functioning” modifying autism, it suggests a life without struggle or without disability; this cannot be further from the truth. The same can be said about the word twice-exceptional, as exceptional is often perceived as “good and outstanding” rather than the intended meaning of rare, not typical. Autism is a difference, but is also a disability when trying to engage with a society that has better communication, emotion recognition, expression, and social interaction skills and does not suffer from sensory sensitivities. In the Swedish Study, suicide was the only specific cause of death showing a higher risk in high-functioning ASD compared with low-functioning ASD[13], and the risk was even higher for females with ASD at 13x the risk of the general population[14].
The Swedish Study was one of the earlier large studies that I could find where a link between higher risk of suicide and suicidal ideation and autism was found. Overall, 83 individuals with ASD in their sample (0.31%) died by suicide, compared with 0.04% of the general population—almost an eight-fold difference[15]. The studies authors identified suicide as one of the top three most common causes of premature mortality among individuals with ASD without co-occurring intellectual disability (ID)[16] what is normally considered high-functioning autism.
The UK Study
This UK Study on suicide and ASD in England indicates a higher prevalence of autism in individuals who died by suicide[17]. The UK Study suggests the need for tailored suicide prevention for autistics and how it is crucial for clinicians to screen for autistic traits and possible undiagnosed autism in patients presenting with suicidal thoughts and behaviours, and to offer appropriate tailored support[18]. The research, based on coroners' inquest records and interviews with next of kin, reveals potential underestimation of suicide rates due to past legal standards of proof regarding cause of death[19]. Key findings include a 10.8% autism prevalence among the deceased when rates of diagnosed autism in the population is generally around 2-3%[20]. This study clearly highlights the importance of considering autism in suicide risk assessments when patterns of suicidal ideation, behaviours and symptoms that are often comorbid with ASD are presented.
This research also demonstrates that both those with clinically diagnosed autism and those that are undiagnosed, but with overlapping autistic traits are significantly more likely to die by suicide[21]. A total of 45% of women with elevated autistic traits...reported making a suicide plan, and 16% had attempted suicide[22]. Only 32% of the sample communicated their suicidal thoughts to another person before they died, and some families reported how the death of their loved one came out of the blue with no obvious warning signs[23].
Additionally the UK Study authors call for a change in environment and the methods and manners in which people with autistic traits are encouraged to seek help[24]. Suicide prevention programs need to consider wider societal issues, such as social exclusion and isolation, poverty, unemployment, trauma and abuse as well as the fact that autistics are often refused assistance as their higher functioning appears to clinicians as “coping” and “functioning”, when it is increasing the risk of suicidal thoughts and other maladaptive behaviours[25].
It should be noted that the UK government has acknowledged the connection between ASD and risk of suicide and added support for studying and developing ASD specific measures to reduce suicide risk in its 5 year plan[26]. In the governmental policy paper on suicide prevention they follow the studies, to say, evidence suggests autistic people, including autistic children and young people, may be at a higher risk of dying by suicide compared with those who are not autistic[27]. They also find it is essential that health, mental health, and local authority services and education providers consider the needs of autistic people in suicide prevention activity[28]. While many actions in this strategy will support autistic people in the UK, all of us in society need to tackle the specific causation factors of suicidality in general, and autism specifically, and tailor support to those that are neurodivergent and struggling versus a one size fits all approach.
Undiagnosed or late-diagnosed autism may be a preventable risk factor for suicide and, therefore, earlier identification and timely access to autism assessment services is vital (emphasis added)[29], [30]. Specific factors that further increase the risk of suicide among autistic people include traumatic, painful life experiences, barriers to accessing support, pressure to ‘camouflage’ or ‘mask’ autism[31] (for example, concealing particular traits that are common in autistic people) and feelings of not belonging[32]. Pressure to conform and to stamp out autistic behaviors that normative viewpoints consider weird or offsetting is contributing to mental health deterioration in autistics and the wider neurodivergent umbrella.

The Utah Kirby study
The Utah Kirby study pulled Utah data over 20 years for those clinically diagnosed with ASD, and demonstrates an elevated risk of death by suicide[33]. Suicide risk in females with ASD diagnosis was over three times higher than in females without ASD[34]. As discussed earlier this study was only for those with a clinical ASD diagnosis (rather than autistic traits), so is limited for those cases where individuals with autism are un or misdiagnosed. The study’s authors also note that suicide determination is given conservatively due to its impact on survivors, which means that there are also suicides that don’t get coded for family, religious, stigma reasons[35]. The authors also mention that it may be particularly difficult in some cases to attribute cause of death with those with ASD as it is more difficult to obtain the “intent” to die[36]. This is similar to the difficulty in knowing intent for whether overdoses are accidental or intentional. Many studies that show a higher 5-10x risk of suicide death, are ones that also include in their studies those with "autistic traits”, or perhaps studies where the participants self-diagnosed/self-report using online tools, rather than solely focusing on clinical diagnoses.
As the Utah Kirby study discusses, the diagnostic criteria for ASD has broadened over time, and ascertainment of accurate ASD diagnosis for those without intellectual disability has improved as well[37]. In other words there is a lost generation of adults that are ASD, but are either never diagnosed or are diagnosed later in their lives[38]. These changes could have affected the observed low incidences in the earlier time periods during which individuals with ASD without ID were likely to be under-ascertained using a community-based, administrative records approach, especially considering the Swedish Study’s[39] finding that suicide in individuals with autism occurred more commonly among those without intellectual disability.
There is evidence that women, especially those with higher cognitive functioning, are often diagnosed with ASD later in life, and some may never receive a formal diagnosis[40]. Therefore, autistic females who died by suicide during the earlier years of this study may have been disproportionately less likely to receive an ASD diagnosis[41]. Females with ASD during the 2013–2017 period, were found to be over five times more likely to die by suicide than their non-ASD peers[42]. The study’s authors noted that the findings related to females with ASD in the most recent time period (2013–2017) are consistent with those of Swedish study[43]. Females with ASD have often been overlooked in research[44] and in unidentified in education and the clinic[45]; the Utah Kirby Study results provide further justification for enhancing focus on females. Some studies have shown that females with ASD may face a variety of challenges including sexual abuse, social difficulties, and conflicts between ASD traits and feminine identity[46]. Traumatic experiences and identity conflicts are known risk factors for suicide in the general population[47]. Further, studies have shown that females may feel the need and have a heightened social ability to “camouflage” or cover-up their autism symptoms[48],[49] with one recent study suggested that these camouflaging behaviors are significantly associated with suicidality in ASD[50]. The Utah Kirby Study also did not differentiate between those with ASD with lower cognitive ability from higher cognitive ability. Studies that have differentiated by cognitive ability in ASD and will be discussed later indicate that the risk of suicide and suicidal ideation is higher for those with higher cognitive functioning and IQ[51],[52].
Meta Studies:
Huntjens Meta Study
This study analyzes the high prevalence of suicidal ideation and attempts in autistic individuals, revealing the need for specialized mental health treatments[53]. This Huntjens analysis estimated the prevalence of suicidal ideation “SI” and suicide attempts “SA” in autistic individuals over a 12-month and a lifetime period across all age groups[54]. Estimates for 12 months (SI: 25.4%, SA: 14.1%) and for lifetime (SI: 37.2%, SA: 15.3%) were consistently higher than the general population’s estimates of (SI: 2.0%, SA 0.3%) over 12 months and (SI: 9%, SA 3%) over a lifetime[55]. The results from this study confirm the substantial magnitude of suicidal thoughts and behaviours in autistics.
Newell - 2023 Meta Study
The Newell 2023 Meta Study reveals a high prevalence of suicidality of both those with a clinical ASD diagnosis and those with autistic traits[56]. Additionally, this study was performed for individuals without intellectual disabilities (above a 70 IQ)[57]. Data from 48,186 participants across 36 studies show pooled prevalence rates of 34.2% for suicidal ideation and 24.3% for suicide attempts, with no significant difference between clinically diagnosed ASD and those individuals with autistic traits[58]. Similar to the Huntjens Meta Study this is significantly higher rates of suicide behaviours than are found in the general population. Cross-national prevalence of suicidal ideation in the general population is approximately 9%, and between 2 and 3% for suicide plans and suicide attempts and behaviours. The risks in the general population are contrasted to those with ASD or autistic traits at 8-12x as high for suicidal attempts and plans[59].
The study’s findings also suggest suicidal ideation is higher in autistic and possibly autistic samples who are transgender or gender non-conforming[60]. This is unsurprising, as transgender and gender non-conforming individuals in the general population exhibit much higher rates of suicidal ideation and suicidal behaviour than their cisgender peers[61]. Along with this, autistic people are more likely to be gender diverse than non-autistic people, and gender-diverse people are also more likely to be autistic[62].
What about those with ASD that have higher functioning cognitive abilities?
For ASD individuals with normal or higher cognitive abilities the risk of premature death by suicide is higher than those that have lower cognitive ability and much higher risk that those without ASD. The risk is even higher in those that are twice-exceptional with both ASD and giftedness, above a 120 IQ.
Carsten Iowa Study
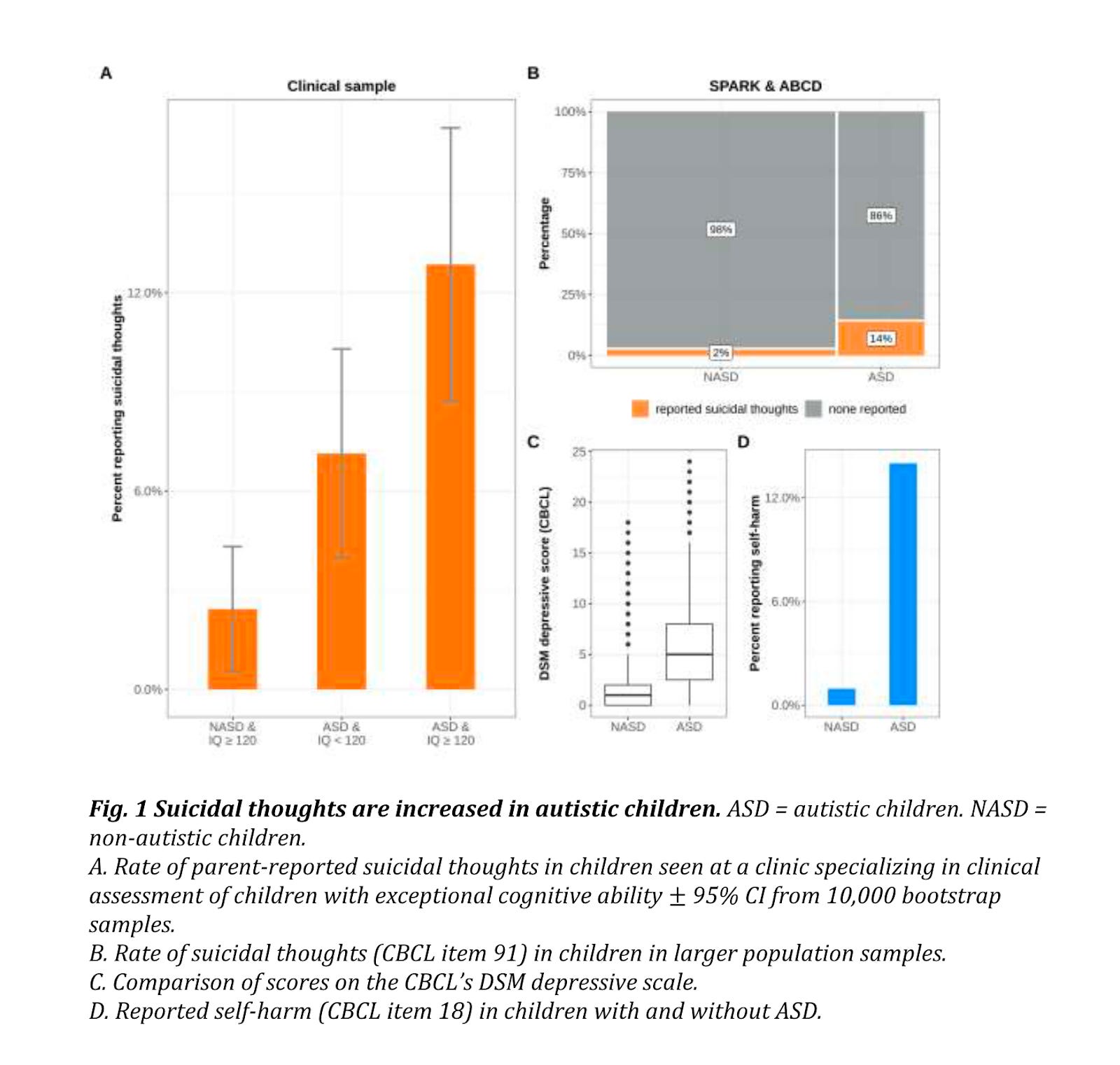
The authors of this study[63] covered the studies that found autism “profoundly increased rates of suicide and depression, in Sweden[64], Japan[65] , Australia[66], meta analysis[67]. The rate of death by suicide has been estimated to be 7.5 times higher in autistic people than those without an autism diagnosis[68]. While rates of suicide death in autistic individuals have varied across samples (0.17 − 0.4% (Kirby[69]; Kõlves[70])) they are consistently higher than rates observed in nonautistic individuals. The increased suicide rate in autism may be partially attributable to a broad increase in depressive symptoms, as autistic people have been shown to have a four-fold increase in lifetime rates of depression[71]. Known protective factors against suicide death, like education, age, and marriage, are not protective in autistic samples (Kõlves[72]). Furthermore, this mental illness burden may be exacerbated by exceptional cognitive ability: in other work, we found that children with an exceptional IQ (≥ 120) and autism have greater feelings of inadequacy and internalizing problems compared to autistic individuals with average IQ[73]. The Carsten Iowa Study findings contrast with research conducted in non-autistic cohorts, where large population studies have found high IQ is a protective factor against suicide death[74], [75], suggesting that the relationship between intelligence and suicide-related traits may vary across diagnostic boundaries”[76]. The Carsten Iowa Study examines the relationship between “exceptional cognitive ability”, autism and suicidality.
Twice-exceptional children (“2E”) are defined as those with both giftedness and a learning disability such as autism, ADHD, dyslexia, etc. The Carsten Iowa study analyzed 2E kids with a diagnosis of autism and high IQ scores >120. For these 2E individuals, they show the highest rate of suicidal thoughts at 12.9%, compared to 2.4% in IQ-matched controls[77]. Additionally, protective factors against suicide death in the general population, like education, age, and marriage, are not protective in autistic samples[78]. Parents of autistic children are found to underreport their child's suicidal ideation[79] and studies would also benefit from a first person perspective[80], [81]. It is often very difficult for parents to know whether their children have suicidal ideation due to difficulties with communication, alexithymia and interoception issues[82], [83]. The results from multiple large samples point toward elevated rates of suicidal thoughts in autism overall, with the highest rates being found in "twice-exceptional" or 2e individuals, i.e., those who were both autistic and had high cognitive ability[84].
The researchers from the Carsten Iowa Study posit that the causes of the increased risk of suicidality in 2E individuals, relate to:
1) In addition to excessive baseline cortisol (think flight or flight adrenal response) linked to autism, it is likely that demonstration of exceptional cognitive ability raises parent, teacher, and peer expectations[85]. Any inability to meet these elevated standards could result in further activation of the hypothalamic-pituitary-adrenal axis, potentially explaining the higher rates of suicidal thoughts we observed in 2e children compared to other autistic children[86].
2) Another mechanism may be found in the relationship between high cognitive ability and "camouflaging"[87], where individuals suppress less socially accepted behavior to fit in. Camouflaging is a universal behavior[88] that has been studied with particular interest in autistic individuals, who engage in this behavior more regularly[89]. In studies of autism, camouflaging has been associated with higher rates of anxiety and depression[90], perhaps due to less support resulting from successful camouflaging, which would tend to delay diagnosis[91]. Consequently, camouflaging in autism is correlated with increased suicidal behavior[92]. Increased cognitive ability may therefore be linked to maladaptive camouflaging that further increases risk for mental health issues in autistic people.[93]
ADHD and Heightened Risk
Individuals with ADHD are also impacted and suffer with higher suicidality[94]. This makes intuitive sense as there appears to be a path toward suicide that is more impulsive in nature[95]. Suicide can appear to an impulsive child to be a permanent solution for a temporary problem. An impulsive ADHDer might attempt suicide on the spur of the moment in response to anger, disappointment, loss, or a whim, where the decision to die by suicide is made within minutes to hours of the attempt[96]. A teen with ADHD may have no intent to die by suicide at the time of his routine follow-up visit where a screening question is asked, but may end his life days or weeks later, on impulse[97].
Undiagnosed ADHD/ASD is linked to a range of negative outcomes, including higher rates of substance abuse, mental health issues, criminal behavior, and lower socioeconomic status[98]. The research demonstrates that identifying ADHD and finding an effective medication improves outcomes and lowers the risk of death, both from suicide and accidental overdose (though it is difficult to impugn intent between accidental and intentional overdoses)[99]. The systemic failure to diagnose ADHD and ASD, leads to a cascade of adverse outcomes that affect not only individuals, but also healthcare, social, and educational systems[100]. There is high overlap between those with both ASD and ADHD, with studies finding 30-50% of those with ASD having ADHD symptoms[101]. Other research is finding even higher rates of up to 75% of those with ASD having ADHD and 15% of the ADHD population having ASD[102].
Combined ADHD and ASD
The combination of autism and ADHD (i.e., dual diagnosis) was made possible in the 2013 DSM-V, prior to which an individual could not be identified as being both ADHDer and autistic[103].
Therefore it is relatively recent that the dual diagnosis of ADHD and ASD was even diagnostically possible. Therefore some studies look to stratify their research into groups of ADHD without ASD traits, and where ADHD individuals also have autistic traits.
As an example is the Blandine French study demonstrates that those children with ADHD+autistic traits experience very severe behavioral, emotional, and educational problems[104]. The combined type of those with ASD and ADHD is often informally referred to as AuDHD and likely comes with its own constellation of heightened risks for lower quality of life, mental illness and earlier mortality[105]. It has been described, being AuDHD is like playing a video game where different people are trying to use the keyboard and the other controls the mouse. Or a more adult description, without censoring for language:

Conclusion:
ASD individuals have a much higher mortality rate from suicide. Those with a high intellectual quotient (IQ) are considered to be at EVEN higher suicidal risk since they tend to not only mask the symptoms of ASD but higher cognitive abilities are also associated with internalizing problems and feelings of inadequacy[106],[107]. The higher IQ and cognitive ability enable more compensation ability for comporting with societal expectations, masking and camouflaging that result in higher suicidality, and internalizing the distress into other conditions, such as anxiety, depression, OCD, etc[108]. Additionally females with ASD in particular are often un and misdiagnosed. These people all need more identification, assessment and support.
Lastly, medical providers, first responders and teachers need specific training on how to support the neurodivergent population. The same interventions that are applied to the neurotypical population cannot be applied to the neurodivergent population, and often cause more harm than good. Neurodivergent people have different brains with different sensory needs. They are prone to more overwhelm. Interventions need to be tailored specifically to support different neurotypes. Neurodivergent individuals need to feel supported in such a way that they are able to “unmask” Autistic individuals need to have their sensory needs supported. Teachers and medical professionals need to learn about autistic burnout[109] and how it is a distinct condition from depression. Many autistic individuals are presenting as suicidal because they are in a state of autistic burnout[110] and our healthcare providers have no idea how to help them. The interventions they are applying are traumatizing them more and making them more suicidal. Schools[111] need to change to be more friendly towards autistic individuals. Early identification[112] is essential for suicide prevention.
ASD, ADHDers and combined AuDHDers may experience difficulty with task initiation, focus, memory, and concentration. Neurodivergents often need more time to process spoken information and respond to questions due to auditory processing speed differences[113]. Allowing ample time for neurodivergents to respond to questions without rushing is critical and necessary to give them time to process the question and answer without scripting an answer as a social avoidance strategy[114]. Additionally, educational and medical practitioners can demonstrate neurodiversity-affirming care by being patient, compassionate, and embracing a non-shaming or judgmental attitude in their interactions and by proactively offering accommodations. The educators, health care providers, and perhaps society at large has a duty to find, effectively treat, accommodate and meet those with sensory, mental health, and processing challenges in the middle. Forcing those that are neurodivergent (a natural state of being), to meet arbitrary societal norms is causing harm. Maybe, to reduce suicidality and mental illness we should all be less hypocrites and more hippocratic.

AFTERWORD
Much of the research cited is open access, though some is not accessible without paid journal credentials. I will try to update this from time to time as new information and research becomes available. I encourage any feedback, edits and suggestions.
________________
[1] Mikle South, Andreia P. Costa & Carly McMorris, Death by Suicide Among People With Autism: Beyond Zebrafish, 4 JAMA Netw. Open e2034018 (2021), https://doi.org/10.1001/jamanetworkopen.2020.34018 (last visited Apr 29, 2024).
[2] Lucas G. Casten et al., The Combination of Autism and Exceptional Cognitive Ability Is Associated with Suicidal Ideation, 197 Neurobiol. Learn. Mem. 107698 (2023), https://www.sciencedirect.com/science/article/pii/S1074742722001228.
[3] Mark Dlugosz, Twice Exceptional: Definition, Characteristics & Identification, Davidson Institute (2021), https://www.davidsongifted.org/gifted-blog/twice-exceptional-definition-characteristics-identification/ (last visited May 1, 2024).
[4] Schindel, B. J., Chen, B. B., Wilcox, H. C., Marvin, A. R., Law, J. K., & Lipkin, P. H. (2024). Suicidal Thoughts and Behaviors Among Children and Adolescents With Autism Spectrum Disorder. JAMA pediatrics.
[5] Benjamin Joffe Schindel et al., Suicidal Thoughts and Behaviors Among Children and Adolescents With Autism Spectrum Disorder, JAMA Pediatr. (2024), https://doi.org/10.1001/jamapediatrics.2024.0207 (last visited Apr 28, 2024).
[6] Id.
[7] Fionnuala Larkin et al., Alexithymia and Intolerance of Uncertainty Predict Somatic Symptoms in Autistic and Non-Autistic Adults, 27 Autism 602 (2023), https://doi.org/10.1177/13623613221109717 (last visited May 6, 2024).
[8] Tatja Hirvikoski et al., Premature Mortality in Autism Spectrum Disorder, 208 Br. J. Psychiatry 232 (2016), https://www.cambridge.org/core/journals/the-british-journal-of-psychiatry/article/prematuremortality-in-autism-spectrum-disorder/4C9260DB64DFC29AF945D32D1C15E8F2 (last visited Apr 26, 2024).
Id.
[9] Hirvikoski et al., supra note 8.
[10] Id.
[11] Id.
[12] Id.
[13] Id.
[14] Id.
[15] Id.
[16] Id.
[17] Sarah Cassidy et al., Autism and Autistic Traits in Those Who Died by Suicide in England, 221 Br. J. Psychiatry 683 (2022), https://www.cambridge.org/core/product/04367C4DD9D8B4B3375A0D25C4764A54.
[18] Id.
[19] Id.
[20] Id.
[21] Id.
[22] Id.
[23] Id.
[24] Id.
[25] Louise Camm-Crosbie et al., “People like Me Don’t Get Support”: Autistic Adults’ Experiences of Support and Treatment for Mental Health Difficulties, Self-Injury and Suicidality, 23 Autism Int. J. Res. Pract. 1431 (2019).
[26] Suicide prevention in England: 5-year cross-sector strategy, GOV.UK, https://www.gov.uk/government/publications/suicide-prevention-strategy-for-england-2023-to-2028/suicide-prevention-in-england-5-year-cross-sector-strategy (last visited Apr 30, 2024).
[27] Cassidy et al., supra note 17.
[28] Suicide prevention in England, supra note 26.
[29] Cassidy et al., supra note 17.
[30] South, Costa, and McMorris, supra note 1.
[31] S. A. Cassidy et al., Is Camouflaging Autistic Traits Associated with Suicidal Thoughts and Behaviours? Expanding the Interpersonal Psychological Theory of Suicide in an Undergraduate Student Sample, 50 J. Autism Dev. Disord. 3638 (2020), http://link.springer.com/10.1007/s10803-019-04323-3 (last visited Apr 30, 2024).
[32] Cassidy et al., supra note 17.
[33] Anne V. Kirby et al., A 20‐year Study of Suicide Death in a Statewide Autism Population, 12 Autism Res. 658 (2019), https://onlinelibrary.wiley.com/doi/10.1002/aur.2076 (last visited Apr 25, 2024).
[34] Anne V Kirby et al., A 20‐year Study of Suicide Death in a Statewide Autism Population, 12 Autism Res. 658 (2019).
[35] Kirby et al., supra note 33.
[36] Id.
[37] Id.
[38] Meng-Chuan Lai & Simon Baron-Cohen, Identifying the Lost Generation of Adults with Autism Spectrum Conditions, 2 Lancet Psychiatry 1013 (2015).
[39] Hirvikoski et al., supra note 8.
[40]Lai and Baron-Cohen, supra note 38.
[41] Kirby et al., supra note 33.
[42] Id.
[43] Hirvikoski et al., supra note 8.
[44] Lai and Baron-Cohen, supra note 38.
[45] Aoife Munroe & Michele Dunleavy, Recognising Autism in Girls within the Education Context: Reflecting on the Internal Presentation and the Diagnostic Criteria, 42 Ir. Educ. Stud. 561 (2023), https://doi.org/10.1080/03323315.2023.2260371.
[46] Sarah Bargiela, Robyn Steward & William Mandy, The Experiences of Late-Diagnosed Women with Autism Spectrum Conditions: An Investigation of the Female Autism Phenotype, 46 J. Autism Dev. Disord. 3281 (2016).
[47] Kirby et al., supra note 33.
[48] Bargiela, Steward, and Mandy, supra note 46.
[49] South, Costa, and McMorris, supra note 1.
[50] Cassidy et al., supra note 31.
[51] Casten et al., supra note 2.
[52] Victoria Newell et al., A Systematic Review and Meta-Analysis of Suicidality in Autistic and Possibly Autistic People without Co-Occurring Intellectual Disability, 14 Mol. Autism 12 (2023), https://doi.org/10.1186/s13229-023-00544-7.
[53] Anne Huntjens et al., The Prevalence of Suicidal Behavior in Autism Spectrum Disorder: A Meta-Analysis., Crisis J. Crisis Interv. Suicide Prev. (2023).
[54] Id.
[55] Id.
[56] Newell et al., supra note 52.
[57] Id.
[58] Id.
[59] Id.
[60] Id.
[61] Id.
[62] Id.
[63] Casten et al., supra note 2.
[64] Hirvikoski et al., supra note 8.
[65] Koji Kato et al., Clinical Features of Suicide Attempts in Adults with Autism Spectrum Disorders, 35 Gen. Hosp. Psychiatry 50 (2013).
[66]Darren Hedley et al., Risk and Protective Factors Underlying Depression and Suicidal Ideation in Autism Spectrum Disorder, 35 Depress. Anxiety 648 (2018).
[67] Chloe C Hudson, Layla Hall & Kate L Harkness, Prevalence of Depressive Disorders in Individuals with Autism Spectrum Disorder: A Meta-Analysis, 47 J. Abnorm. Child Psychol. 165 (2019).
[68] Hirvikoski et al., supra note 8.
[69] Kirby et al., supra note 33.
[70] Kairi Kõlves et al., Assessment of Suicidal Behaviors Among Individuals With Autism Spectrum Disorder in Denmark, 4 JAMA Netw. Open e2033565 (2021), https://doi.org/10.1001/jamanetworkopen.2020.33565 (last visited May 1, 2024).
[71] Hudson, Hall, and Harkness, supra note 67.
[72] Kõlves et al., supra note 70.
[73] Jacob J. Michaelson et al., Autism in Gifted Youth Is Associated with Low Processing Speed and High Verbal Ability, medRxiv 2021.11.02.21265802 (2022), http://medrxiv.org/content/early/2022/03/02/2021.11.02.21265802.abstract.
[74]Ian J. Deary, Alexander Weiss & G. David Batty, Intelligence and Personality as Predictors of Illness and Death: How Researchers in Differential Psychology and Chronic Disease Epidemiology Are Collaborating to Understand and Address Health Inequalities, 11 Psychol. Sci. Public Interest 53 (2010), https://doi.org/10.1177/1529100610387081 (last visited May 7, 2024).
[75] A. Sörberg Wallin et al., Suicide Attempt Predicted by Academic Performance and Childhood IQ: A Cohort Study of 26 000 Children, 137 Acta Psychiatr. Scand. 277 (2018), https://doi.org/10.1111/acps.12817 (last visited May 7, 2024).
[76]Casten et al., supra note 2.
[77] Id.
[78] Id.
[79] L. O’Halloran, P. Coey & C. Wilson, Suicidality in Autistic Youth: A Systematic Review and Meta-Analysis, 93 Clin. Psychol. Rev. 102144 (2022).
[80] Casten et al., supra note 2.
[81] Lucy Anne Livingston, Punit Shah & Francesca Happé, Compensatory Strategies below the Behavioural Surface in Autism: A Qualitative Study, 6 Lancet Psychiatry 766 (2019).
[82] Michael V. Lombardo et al., Self-Referential Cognition and Empathy in Autism, 2 PloS One e883 (2007).
[83] Laura Crane et al., ‘Something Needs to Change’: Mental Health Experiences of Young Autistic Adults in England, 23 Autism 477 (2019), https://doi.org/10.1177/1362361318757048 (last visited May 7, 2024).
[84] Casten et al., supra note 2.
[85] Id.
[86] Id.
[87] Livingston, Shah, and Happé, supra note 81.
[88] Courtney Jorgenson et al., Social Camouflaging in Autistic and Neurotypical Adolescents: A Pilot Study of Differences by Sex and Diagnosis, 50 J. Autism Dev. Disord. 4344 (2020).
[89] Julia Cook et al., Camouflaging in Autism: A Systematic Review, 89 Clin. Psychol. Rev. 102080 (2021), https://www.sciencedirect.com/science/article/pii/S0272735821001239.
[90]Laura Hull et al., Is Social Camouflaging Associated with Anxiety and Depression in Autistic Adults?, 12 Mol. Autism 13 (2021).
[91] Goldie A. McQuaid, Nancy Raitano Lee & Gregory L. Wallace, Camouflaging in Autism Spectrum Disorder: Examining the Roles of Sex, Gender Identity, and Diagnostic Timing, 26 Autism Int. J. Res. Pract. 552 (2022).
[92] Cassidy et al., supra note 31.
[93] Casten et al., supra note 2.
[94] Lin Li et al., ADHD Pharmacotherapy and Mortality in Individuals With ADHD, 331 JAMA 850 (2024), https://doi.org/10.1001/jama.2024.0851 (last visited May 4, 2024).
[95] Fatima Malik et al., Missed Opportunities for Suicide Prevention in Teens with ADHD, 12 J. Affect. Disord. Rep. 100482 (2023), https://linkinghub.elsevier.com/retrieve/pii/S2666915323000215 (last visited May 1, 2024).
[96] Id.
[97] Id.
[98]Blandine French et al., Risks Associated With Undiagnosed ADHD and/or Autism: A Mixed-Method Systematic Review, 27 J. Atten. Disord. 1393 (2023).
[99] Li et al., supra note 94.
[100] Blandine French et al., Risks Associated With Undiagnosed ADHD and/or Autism: A Mixed-Method Systematic Review, 27 J. Atten. Disord. 1393 (2023).
[101] Naomi Ornstein Davis & Scott H. Kollins, Treatment for Co-Occurring Attention Deficit/Hyperactivity Disorder and Autism Spectrum Disorder, 9 Neurother. J. Am. Soc. Exp. Neurother. 518 (2012).
[102] Gagan Joshi & Timothy E. Wilens, Pharmacotherapy of Attention-Deficit/Hyperactivity Disorder in Individuals with Autism Spectrum Disorder, 31 Child Adolesc. Psychiatr. Clin. N. Am. 449 (2022).
[103] Regina Taurines et al., ADHD and Autism: Differential Diagnosis or Overlapping Traits? A Selective Review, 4 Atten. Deficit Hyperact. Disord. 115 (2012).
[104] Amelia Kotte et al., Autistic Traits in Children with and without ADHD, 132 Pediatrics e612 (2013).
[105] Siân Boyle, The Sudden Rise of AuDHD: What Is behind the Rocketing Rates of This Life-Changing Diagnosis?, The Guardian, Apr. 4, 2024, https://www.theguardian.com/lifeandstyle/2024/apr/04/audhd-what-is-behind-rocketing-rates-life-changing-diagnosis (last visited May 8, 2024).
[106] Casten et al., supra note 2.
[107] Mayank Gupta, Nihit Gupta & Theodore Petti, Autism and Suicide: Strategies to Dovetail Emerging Evidence in Child and Adolescent Suicide Risk Assessments, (2023), https://www.researchsquare.com/article/rs-3590767/v1 (last visited May 1, 2024).
[108] Cassidy et al., supra note 31.
[109] 14d85f_824e9f7c7ed24b2c861cb4c497f72c6e.pdf, https://www.autisticadvocate.co.uk/_files/ugd/14d85f_824e9f7c7ed24b2c861cb4c497f72c6e.pdf (last visited May 7, 2024).
[110] Dora M. Raymaker et al., “Having All of Your Internal Resources Exhausted Beyond Measure and Being Left with No Clean-Up Crew”: Defining Autistic Burnout, 2 Autism Adulthood 132 (2020), https://doi.org/10.1089/aut.2019.0079 (last visited May 2, 2024).
[111] Walk In My Shoes, (2020),
(last visited May 7, 2024).
[112] Emily Katy: “Finding out I was autistic saved my life,” https://www.bbc.com/news/uk-england-beds-bucks-herts-68600388 (last visited May 7, 2024).
[113] L Cobbaert & A Rose, Eating Disorders and Neurodivergence: A Stepped Care Approach, Eat. Disord. Neurodiversity Aust. (2023).
[114] Id.